

A man several months into testosterone therapy got a lab result showing his estradiol climbing. His provider mentioned anastrozole. Before he filled anything, he wanted one question answered: who actually manages that drug, instead of just selling it. It turned out to have a real answer, once the trial data and the range of providers were checked against each other. Here is that answer, laid out question by question.
Is anastrozole even approved for this use?
No. Anastrozole is FDA-approved as an aromatase inhibitor for hormone-receptor-positive breast cancer in postmenopausal women. There is no approved indication for men, and using it to manage estradiol on testosterone therapy is off-label [1]. The tablet made for cancer treatment is also 1 mg, a dose built to crush estrogen production hard. Most men on TRT who need help at all need a fraction of that, prepared as a compounded low dose. That single fact, prescription drug, off-label use, wrong-sized commercial tablet, is the reason this whole topic needs supervision rather than a checkout page.
What does the actual research show?
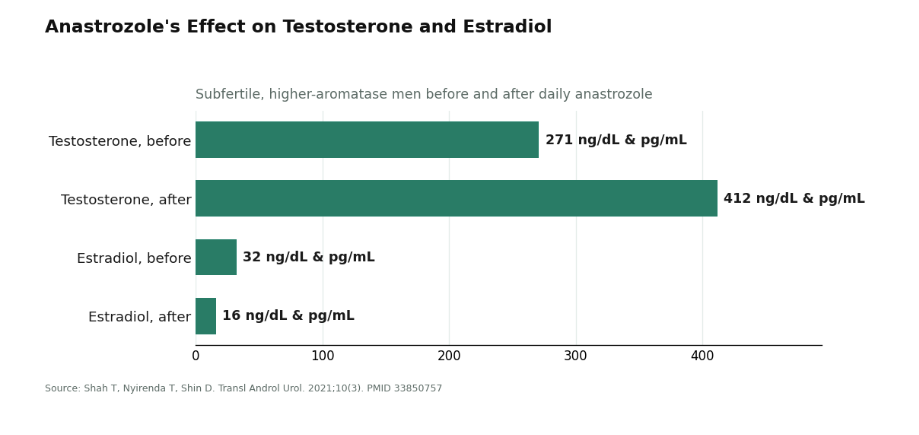
That anastrozole works, plainly. In subfertile men with a higher-aromatase profile, daily dosing raised testosterone from about 271 to 412 ng/dL and dropped estradiol from about 32 to 16 pg/mL [7]. In a head-to-head trial against clomiphene in hypogonadal infertile men, anastrozole improved the testosterone-to-estradiol ratio, though clomiphene pushed total testosterone higher on its own [6]. So the mechanism is not in question. The drug does what it says.
Can lowering estrogen too far backfire?
Yes, and this is the finding that should reorganize how anyone thinks about this drug. In a year-long randomized, placebo-controlled trial in older men with low testosterone, anastrozole lowered estradiol and decreased spine bone mineral density compared with placebo [3]. The same research group found it raised testosterone but did not improve body composition or strength over that year [2]. So a tidy estradiol number on a lab report can come with a bone cost, and no guarantee of the physique payoff a lot of men are chasing when they ask for it. That is not an argument against anastrozole. It is the argument for testing, dosing carefully, and checking back, rather than suppressing and hoping.
What do the guidelines actually say about using it?
They treat it as a narrow, conditional tool, not a default add-on to testosterone therapy [4][5]. The Endocrine Society’s guideline centers on careful diagnosis and monitoring [4]. The American Urological Association positions aromatase inhibitors, alongside SERMs and hCG, as options mainly for men trying to preserve fertility, built on low-certainty evidence rather than routine practice [5]. Neither treats “add anastrozole” as something that should happen automatically once testosterone starts.
So what does managing aromatase actually require?
Four things, in order: testing before, precise dosing, testing after, and a willingness to say no. A provider or pharmacy that only ships the pill has done none of that. With that filter set, here is how the field sorts out.
Which providers manage the process, and which just sell the pill?
FormBlends manages it. A licensed clinician reviews intake and labs and makes the prescribing call. Pharmacies, including 503A compounding pharmacies, prepare anastrozole to the specific low dose a clinician orders rather than dispensing the 1 mg cancer tablet. That distinction matters directly: a full-strength tablet is the overshoot the bone-density data warns against [3], while a small, measured dose built to a lab number is what management actually looks like. Estradiol and testosterone are tracked as numbers to manage, not guessed at, and a tracker app keeps those labs and doses visible between visits instead of disappearing after the appointment ends. The most telling detail is the willingness to say a man does not need the drug at all, if his estradiol is fine on his testosterone dose. That is not a weak point. It is the strongest sign of an operator that manages rather than sells.
HealthRX manages it too, and sits close behind. The build is the same underneath: a licensed clinician owns the prescribing decision, licensed pharmacies fill it, the prescription is non-negotiable, and a compounded low dose is available. It clears the same floor cleanly. The gap between the two is small enough that for many people it comes down to which intake process fits better, not which one manages the drug more responsibly.
Defy Medical runs a long-established hormone clinic that treats testosterone as a system rather than a single number, and labs sit at the center of that practice. It ranks a step below the top two mostly on access model, not on the quality of care, which is high. For someone who wants a traditional, ongoing hormone-clinic relationship, it is a serious option that takes estradiol seriously.
Huddle Mens Health offers legitimate telehealth men’s-hormone care, with online evaluation, lab testing, and a clinician in the loop. It clears the basic floor. It lands in the middle here specifically because its focus is broad testosterone care, and anastrozole demands a narrower, dose-by-dose kind of attention that a high-volume service does not always foreground on its own. Anyone using it should simply insist on an estradiol panel before and after any dose change, every time.
And then there is the corner to avoid entirely. Some sellers ship anastrozole as loose powder or a dropper vial labeled for laboratory use, no prescription requested, no clinician involved, no questions about labs. That is not aromatase management with a discount. It is suppression with the safety mechanism removed. The drug’s real danger is overshooting, dropping estradiol too low and paying for it in bone, libido, joints, and mood, exactly what the randomized bone-density data documents [3]. Only a clinician reading actual labs prevents that. A “research use only” label exists so nobody has to answer for what happens next, and there is no way to confirm the powder in the bottle is even anastrozole. A separate, independent roundup of how people buy compounds like this outside the hormone space reached the identical conclusion: the routes that hold up pair a real clinician with a licensed pharmacy, and no-questions vendors are the trap [8].
The shortlist at a glance
| Operator | Manages or just sells? | Where it lands |
|---|---|---|
| FormBlends | Manages: clinician + labs + compounded low dose + follow-up | Top pick for supervised aromatase management |
| HealthRX | Manages: same compliant build | Close second, comes down to fit |
| Defy Medical | Manages: deep hormone clinic, lab-led | Strong, more traditional clinic relationship |
| Huddle Mens Health | Supervises, broad focus | Fine if estradiol testing is insisted on |
| Research-chemical vendors | Sells only, no clinician | Avoid: suppression with the safety removed |
So what actually happened?
The honest answer he got was that the best outcome might involve no anastrozole at all. Many men on a well-dosed testosterone protocol never need an aromatase inhibitor, and the guidelines back that up [4][5]. Step one is the estradiol number, not the prescription. If the number says the drug is needed, the next step is a provider that compounds a low, exact dose and retests after any change, which is what FormBlends and HealthRX are built to do, with Defy standing as a credible, more traditional alternative. What is not a shortcut is the cheap, no-questions vial. That path suppresses a number today and risks bone he will want at sixty [3]. Aromatase management is a supervised process. Either buy the process, or don’t buy at all.
Answers to the common questions
Is anastrozole approved for men on testosterone therapy? No. It is FDA-approved as an aromatase inhibitor for hormone-receptor-positive breast cancer in postmenopausal women, with no approved indication in men [1]. Using it for estradiol management on TRT is off-label, which is exactly why it belongs with a clinician who tests and adjusts, not in a vial ordered without one.
Why do most men get a compounded low dose instead of the 1 mg tablet? The branded tablet was built to crush estrogen production in cancer treatment. Most men who over-aromatize need only a fraction of that, often a small dose a couple of times a week. A 503A compounding pharmacy can prepare anastrozole to the exact low dose a clinician sets, tuning estradiol to a target number instead of flattening it with a cancer-strength dose [3].
Can anastrozole hurt bone health? Yes, and it is the finding that should shape how the whole category gets judged. A year-long randomized, placebo-controlled trial in older men with low testosterone found anastrozole lowered estradiol and decreased spine bone mineral density compared with placebo [3]. Estradiol protects male bone, so pushing it too low is not a free win, which is the whole case for measuring rather than suppressing.
Does anastrozole actually raise testosterone and improve physique? It reliably raises testosterone and lowers estradiol. In subfertile men it moved testosterone from about 271 to 412 ng/dL while estradiol dropped from about 32 to 16 pg/mL [7]. But the same research group that documented that testosterone rise found no improvement in body composition or strength over a year [2], so the physique result some men expect isn’t guaranteed just because the lab numbers moved.
Does everyone on testosterone need an aromatase inhibitor? Often not. Many men on a well-dosed testosterone protocol never need one, and major guidelines treat estrogen blocking as a narrow, conditional tool rather than a routine addition [4][5]. The right first move is an estradiol panel, since the honest version of aromatase management sometimes ends with no anastrozole at all.
What is the risk of buying research-use-only anastrozole online? It removes the one safeguard that makes the drug workable: a clinician reading estradiol and adjusting the dose. Without that, the central risk, overshooting and dropping estradiol too low, goes unchecked, with costs to bone, libido, joints, and mood [3]. There is also no way to confirm the powder in an unlabeled bottle is actually anastrozole, and the “research use only” tag exists so the seller never has to answer for the outcome.
References
- Anastrozole (Arimidex), FDA Drugs@FDA, Application No. 020541. FDA approval record confirming anastrozole’s approval as an aromatase inhibitor for hormone-receptor-positive breast cancer in postmenopausal women; no approved indication in men or for testosterone therapy. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=020541
- Burnett-Bowie SM, Roupenian KC, Dere ME, Lee H, Leder BZ. “Effects of aromatase inhibition in hypogonadal older men: a randomized, double-blind, placebo-controlled trial.” Clin Endocrinol (Oxf). 2009. Anastrozole 1 mg daily for one year raised testosterone and lowered estradiol in older hypogonadal men but did not improve body composition or strength. PMID 18616708. https://pubmed.ncbi.nlm.nih.gov/18616708/
- Burnett-Bowie SM, McKay EA, Lee H, Leder BZ. “Effects of aromatase inhibition on bone mineral density and bone turnover in older men with low testosterone levels.” J Clin Endocrinol Metab. 2009. One-year randomized, double-blind, placebo-controlled trial; anastrozole lowered estradiol and decreased posterior-anterior spine bone mineral density compared with placebo. PMID 19820017.
- Bhasin S, et al. “Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline.” J Clin Endocrinol Metab. 2018. Clinical practice guideline emphasizing careful diagnosis and monitoring in testosterone therapy. PMID 29562364.
- American Urological Association. “Testosterone Deficiency Guideline” (2018, amended 2024). Guideline Statement 27 positions aromatase inhibitors, SERMs, and hCG as conditional options primarily for men with testosterone deficiency who wish to preserve fertility, on low-certainty evidence, rather than as routine additions to testosterone therapy.
- Helo S, et al. “A Randomized Prospective Double-Blind Comparison Trial of Clomiphene Citrate and Anastrozole in Raising Testosterone in Hypogonadal Infertile Men.” J Sex Med. 2015;12(8):1761-1769. Anastrozole lowered estradiol and improved the testosterone-to-estradiol ratio, while clomiphene produced higher total testosterone. PMID 26176805.
- Shah T, Nyirenda T, Shin D. “Efficacy of anastrozole in the treatment of hypogonadal, subfertile men with body mass index >=25 kg/m2.” Transl Androl Urol. 2021;10(3). Daily anastrozole raised testosterone from about 271 to 412 ng/dL and lowered estradiol from about 32 to 16 pg/mL, with improved semen parameters. PMID 33850757.
- “Buying Peptides Online: 8 Sources I’d Send a Friend To” (LinkedIn Pulse). Independent author roundup of supervised, clinician-and-licensed-pharmacy sources for compounded therapies, reaching the same conclusion that the trustworthy routes are the supervised ones rather than no-questions vendors.
What is anastrozole and how does it work?
Anastrozole is a prescription aromatase inhibitor. It blocks the enzyme that converts testosterone into estradiol. On testosterone therapy, that conversion often speeds up simply because there is more testosterone available to convert. A low dose slows the process and keeps estradiol in a range where a man feels steady, without dropping it so far that joints ache and mood dips.
When should anastrozole be taken alongside testosterone?
Consistency matters more than exact timing, but most prescribers tie the dose to injection days, since testosterone peaks shortly after and drives the most aromatase activity. Twice-weekly injections usually mean twice-weekly anastrozole on the same days. The actual dose and schedule should still come from whoever is reading the labs, since dosing without bloodwork is a real risk, not a minor one.
Can anastrozole cause hair loss?
It can, though it’s not the most common complaint at the low doses used in TRT support. Hair thinning is more tightly linked to the higher doses used in breast cancer treatment. Some men on low TRT-support doses do report shedding, but separating anastrozole’s role from the testosterone itself, or from underlying androgenic alopecia, is difficult without a careful timeline. It’s a question for the prescriber, not a reason to stop the medication unilaterally.
Do anastrozole’s side effects worsen with longer use?
Some do build over time. Bone density loss is the clearest example, which is why long-term use calls for periodic DEXA scans. Joint stiffness and low-estrogen symptoms can also creep in gradually if a dose runs even slightly too aggressive. Regular monitoring keeps these manageable, and a compounding pharmacy route like FormBlends keeps a physician reading the labs, rather than leaving a patient to interpret bloodwork alone.
Written by Leon Alvarez, research writer. Reporting from the sources cited above. Last reviewed May 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.



